

Admin Name
1 year ago
admin
#emergency
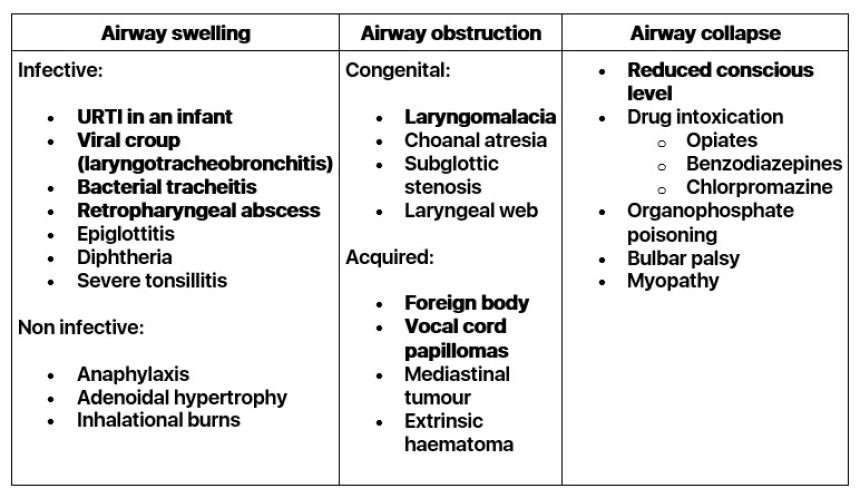
Airway Obstruction
Causes (common causes in bold)
 Important points in history
Important points in history- Length of history of stridor (Stridor since birth suggests a congenital anomaly)
- Present all the time or only when upset / feeding / lying down?
- Coryzal symptoms
- Fever
- Barking cough, hoarse voice (suggests croup)
- Sudden onset when playing or history of choking (suggests foreign body)
- Recurring episodes (suggests vocal cord papilloma)
- Pain on swallowing (suggests retropharyngeal abscess)
- Ingestion of drug or food (suggests allergy or poisoning)
- Immunization history
- HIV status (suggests Kaposi's sarcoma or laryngeal papillomas)
- Toxic, shock, temperature (suggests epiglottitis)
- Hoarse voice, barking cough (suggests croup)
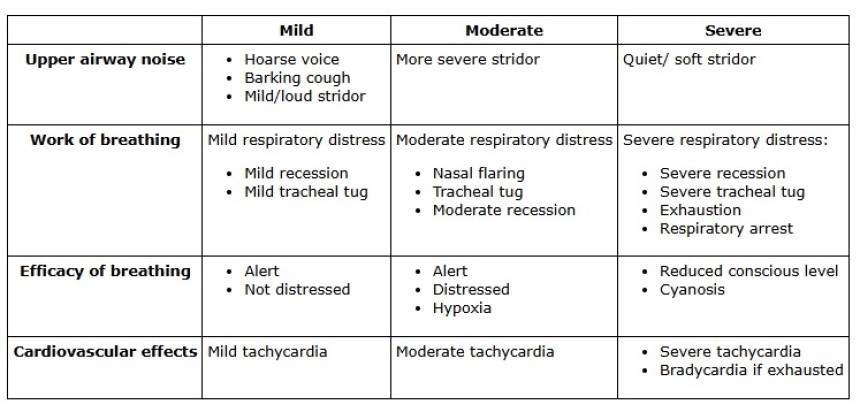
- Severity of respiratory distress / central cyanosis
- Agitation/ drowsiness
- Respiratory rate/ heart rate
- Drooling (suggests epiglottitis, retropharyngeal abscess)
- Posture - e.g. sitting up, leaning forward
- Unilateral hyperexpansion or wheeze (suggests foreign body)
- Bull neck appearance, blood stained nasal discharge, grey pharyngeal membrane (suggest diphtheria)
- Associated urticaria or lip swelling (suggests naphylaxis)
- Facial burns, singed nasal hairs, oral/ nasal soot (suggests inhalational burn)
Remember: The loudness of the stridor does not reflect the severity of the airway obstruction
 Investigations
InvestigationsRemember: Avoid painful/ frightening procedures (including MPS & PCV) until airway is stable or secureIf query croup/ epiglottitis no investigations required, check SaO2
If query foreign body/ tumour/ retropharyngeal abscess - CXR, lateral neck X-ray
- CXR - May see foreign body if radio-opaque
- Unilateral hyper-expansion suggests FB in main bronchus with air-trapping
- If a coin seen above the carina:
- Seen as a circle - likely in the oesophagus
- Seen as a straight line - likely between the vocal chords
- Lateral neck - retropharyngeal abscess: distance between the anterior vertebral body wall and the air column in the pharynx is increased (at C3 this distance should be no more than 1/2 of the vertebral body diameter).
- If query toxic - blood culture ONLY once airway stable.
- All but the mildest case of croup will need to be admitted.
- If severe upper airway obstruction d/w senior/ anaesthetist about admittion to ICU.
- TRY AND KEEP CHILD CALM - let child sit on parent's knee
- Severe obstruction: Nebulised adrenaline (1-2ml 0f 1:1000 in 2mls of saline), dexamethasone (0.6mg/kg, max 10mg) or prednisolone (2mg/kg), call for senior help (registrar, consultant, anaesthetist, ENT)
- Croup oxygen, steroids (dexamethason 0.6mg/kg or prednisolone 2mg/kg), adrenaline nebuliser if indicated.
- Bacterial infection (tracheitis, retropharyngeal abscess): ceftriaxone
- Foreign body: call ENT/ surgeons for bronchoscopy
- Epiglottitis: keep calm, oxygen, call for senior support - needs transfer to ICU for intubation. DO NOT EXAMINE THROAT, OR PUT IN AN IV LINE OR DO ANY BLOOD TESTS.
- Anaphylaxis: see anaphylaxis protocol
- Laryngomalacia: usually resolves as child gets older
- Ensure adequate analgesia, fluid and nutritional intake.
- Admit to HDU
- Inform senior about every child that requires adrenaline nebulisers
- If transferred from ICU monitor closely for deterioration
- When child fully recovered and no longer has respiratory distress 12 hours after last adrenaline nebulisation.




